![]() Lymphoma consultants have joined forces to establish a national network aimed at improving patient care. In New Zealand, lymphoma patients may be treated by a haematologist, medical oncologist or radiation oncologist, depending on their location, the lymphoma subtype they have and the stage of the disease. As the three groups of specialists rarely meet nationally, knowledge is seldom shared.
Lymphoma consultants have joined forces to establish a national network aimed at improving patient care. In New Zealand, lymphoma patients may be treated by a haematologist, medical oncologist or radiation oncologist, depending on their location, the lymphoma subtype they have and the stage of the disease. As the three groups of specialists rarely meet nationally, knowledge is seldom shared.
The incidence of lymphoma is rising. We are seeing increasing numbers of patients with this disease, approximately 900 patients a year are diagnosed in New Zealand.
We believe that we can achieve a great deal by collaborating and exchanging information. The field of lymphoma has been expanding fast in all aspects: diagnosis, prognosis, management and long term follow up. Lymphoma is more prevalent now worldwide, and we are seeing older patients being treated more aggressively and patients are living longer. For the above reasons, there is a great need for collaboration and support between clinicians, nurses and patients. The New Zealand Lymphoma Network was hence established in 2008, sponsored by Leukaemia & Blood Cancer New Zealand.
Our aim is for haematologists, oncologists and radiation oncologists in New Zealand to meet regularly to exchange knowledge, review the literature, discuss and establish national treatment protocols. We aim to work towards establishing a national database for lymphoma patients, collaborate nationally and with other international groups on clinical trials and molecular research, collaborate with patients support groups like Leukaemia & Blood Cancer New Zealand and to lobby for the introduction of new management modalities (drugs, investigations) in lymphoma.
Our aim is to improve our lymphoma patients’ care and ultimately develop our own protocols through multidisciplinary prospective trials and retrospective analysis from our existing data.
The group has identified a range of issues to pursue including:
• National guidelines for the treatment of lymphoma
• Guidelines regarding referral for bone marrow transplantation, radiotherapy and new innovations in imaging like positron emitting tomography (PET) scan
• More support for patients and families
• Lobbying to introduce and fund new targeted therapies
• Greater involvement of New Zealand patients in clinical trials
• Psychosocial effects of lymphoma – ranging from financial troubles to stress, depression and fatigue.
It is envisaged that the network will also share knowledge with international groups as it evolves further.
The management of patients with lymphoma requires a multi disciplinary approach with input from physicians, nurses and organisations like LBC. This will enable issues related to the possible complications of chemo and radiotherapies, including fertility, and secondary cancers to be addressed.
Further aims are to enrol patients in clinical trials. It is through these local, national and international trials, that patients can access new drugs and be closely monitored and to start a national database to preserve information on patients and treatments.
The Lymphoma Network also allows treatment groups to share information, pose questions about difficult cases and offer us the opportunity to support each other.
Samar Issa, FRACP, FRCPA
Consultant Haematologist
Head of Lymphoma Service
Middlemore Hospital
Lymphoma is not one cancer but refers to many different malignancies which all originate from lymphocytes, which are white blood cells that play an important role in our immune system. Humans have 3 main types of lymphocytes: T-cells, B-cells and NK cells, however within each of these groups many subsets of lymphocytes are defined, an of which may cause lymphoma.
Overall lymphoma is a relatively common cancer, diagnosed in approximately 800 New Zealanders every year; however some lymphomas are very rare. Immune suppression, autoimmune diseases, ageing, ethnicity, radiation exposure and certain infections (viral and bacterial are known to predispose to some types of lymphomas; however in most patients no cause for their lymphoma is identified. Familial (i.e. genetic or inherited) lymphomas are rare.
Lymphoma can arise in any part of the body, although usually lymph nodes are involved. Patients can present with a huge variety of signs and symptoms which can often mimic other diseases; therefore recognising lymphoma can be challenging and patients are occasionally frustrated by multiple tests and a delay in diagnosis. Conversely, many patients with low grade lymphomas have no symptoms and enlarged lymph nodes are found incidentally when scans or blood tests are performed for other indications.
A definitive diagnosis of lymphoma is made by performing several types of tests on a biopsy of the involved tissue. Over 50 types of lymphoma are known, and as the treatment and prognosis of each type of lymphoma may vary considerably, it is vital to obtain an accurate diagnosis. When a diagnosis of lymphoma is established, staging investigations determine the extent of lymphoma throughout the body. Staging contributes to treatment planning and helps predict outcome. Staging investigations include a “full body” CT scan, bone marrow biopsy, and blood tests – including testing for some viral infections. Occasionally special scans (such as MRI or PET) or a lumbar puncture may be required. Unlike other types of cancer it is not only the stage which predicts prognosis and in some case even very advanced disease is considered curable.
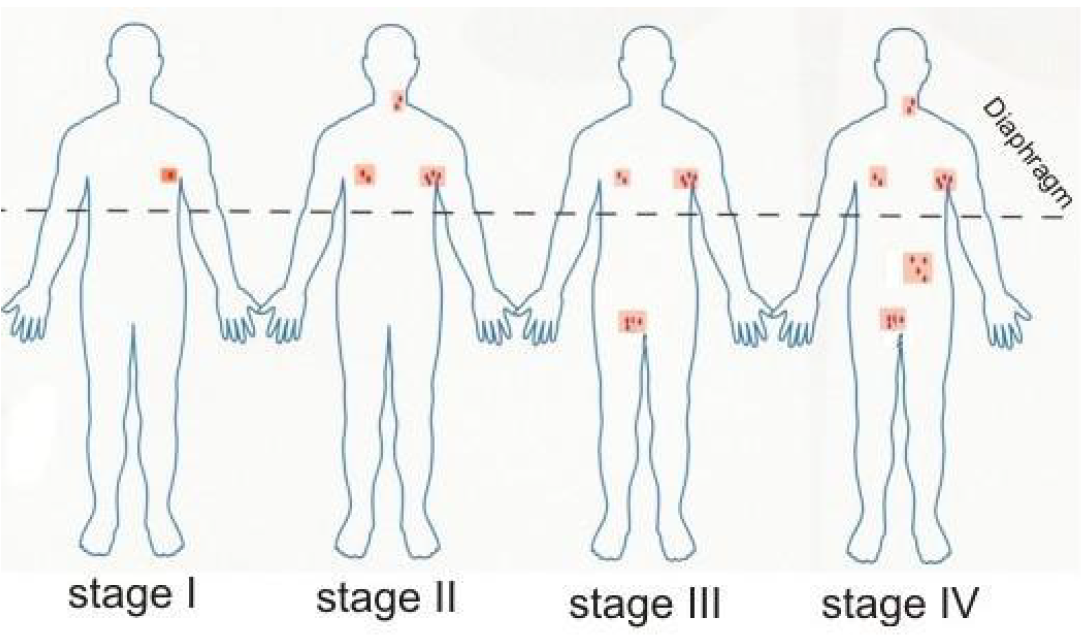
Lymphoma staging:
Stage I Single nodal area or structure
Stage II Two or more nodal areas on the same side of the diaphragm
Stage III Nodal areas on both sides of the diaphragm
Stage IV Extranodal involvement
B Symptoms Fever >38°C, weight loss >10% in the preceding 6 months, drenching night sweats
The type of lymphoma/biopsy results, staging investigations and patient’s overall heath determine the treatment options, which may include monitoring only (for low grade disease), radiotherapy, chemotherapy, bone marrow/stem cell transplant and supportive care (such as blood transfusions). Some types of lymphomas have high cure rates while others are considered incurable. Many lymphomas have a validated prognostic scoring system which can help in predicting outcomes.
Lymphoma classification:
There are several components to lymphoma classification. The following information is not exhaustive but outlines the basic framework for classification. Comprehensive diagnostic criteria for lymphoma have been published by the World Health Organisation.
1. The type of lymphocyte involved: In Hodgkin lymphoma, unique malignant B-lymphocytes called Reed-Sternburg and Hodgkin cells are seen. These cells are not found in any other types of lymphomas, which are therefore referred to as non-Hodgkin lymphomas (NHL). NHL is further classified as to the type of lymphocyte involved e.g. B-cell vs T-cell.
2. The site of lymphoma: For example, central nervous system lymphoma or cutaneous (skin) lymphoma
3. The rate of growth: Although there are exceptions to this rule, typically fast growing or aggressive tumours are composed of large lymphoma cells, while slow growing or indolent lymphomas are most often composed of small cells.
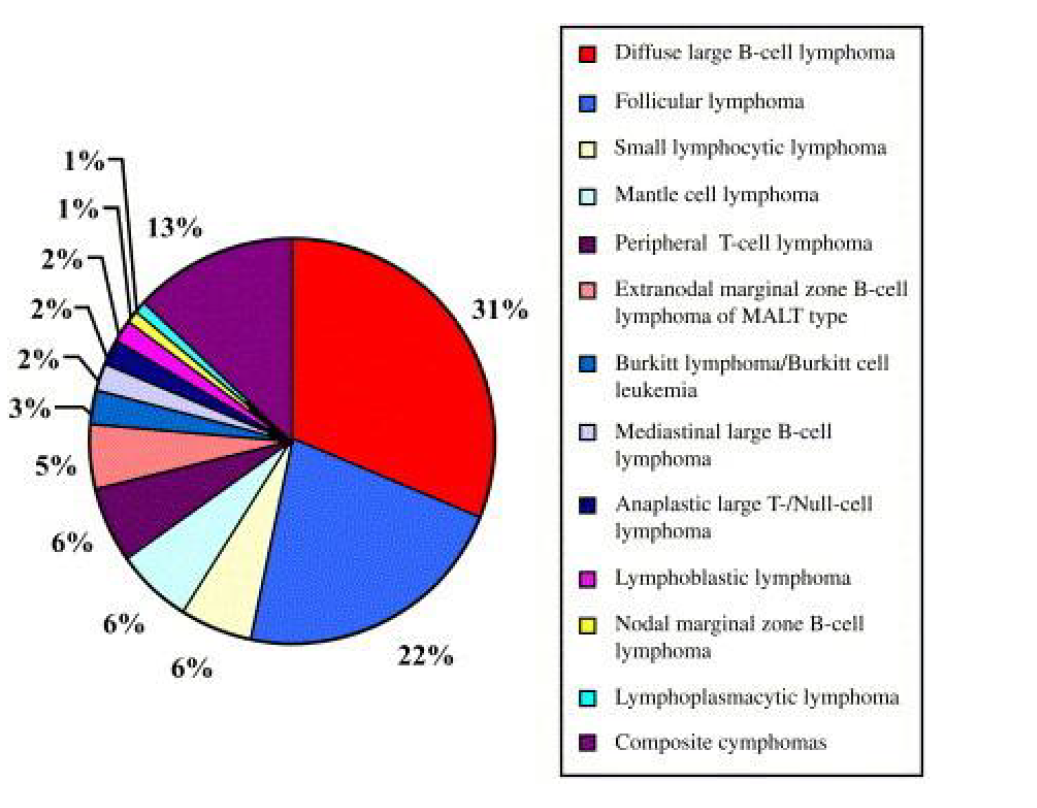
B-cell non-Hodgkin lymphomas are the most common types of lymphoma, in particular follicular lymphoma, (an indolent lymphoma) and diffuse large B-cell lymphoma, an aggressive lymphoma.
Frequencies of the more common subtypes of non-Hodgkin lymphoma:
Hodgkin Lymphoma
Hodgkin lymphoma, although, less common than other lymphomas, has its own unique aspects. Typical presentations are enlarged lymph nodes in the neck or within the chest. About 20% of patients also have fevers, sweats or skin itch at the time of diagnosis.
The requirement to biopsy the enlarged nodes and perform CT scans and bone marrow biopsies, in some cases, is similar to other lymphomas.
Hodgkin lymphoma occurs more frequently in younger patients than other lymphomas posing unique issues relating to preservation of fertility and minimizing the long term side effects of treatment. Fortunately, current treatment using combination chemotherapy and radiotherapy has a high cure rate and fertility is usually preserved. Clinical trials are currently focusing on minimizing treatment in good risk disease and intensifying treatment in poor risk disease. Patients with recurrent disease may still be cured with an autologous stem cell transplant.
More information
For more information about the different subtypes of lymphoma, including patient information booklets, please click here.
There is a list of clinical trials currently available in New Zealand in lymphoma, available on the “ClinTrial Refer” app.
Android Device click here
Apple App Store click here
Tissue banking
Tissue banks (also known as tumour banks) are a useful research resource. They collect, process, store and subsequently provide cancerous tissues and cells (including blood and bone marrow) for ethically approved research studies. This may be in the form of solid tumours (e.g. lymphoma or breast cancer), bone marrow and blood (e.g. leukaemia, myeloma) that is being collected in a routine biopsy or blood test.
Specially trained medical professionals will provide you with full information regarding the tissue bank, obtain informed consent, collect and prepare the samples for storage as well as record comprehensive, de-identified, clinical information about each donor and the corresponding sample(s). Tissue banks have become an integral part of many state-of-the-art hospitals and cancer centres across the world.
The tumour samples and associated clinical data are important resources for scientists engaged in molecular research to develop better diagnostic tools and new drug therapies. Results from this type of research have been successful in recent times leading to the development of targeted therapies such as Imatinib (also known as Glivec, for chronic myeloid leukaemia) and Rituximab (also known as MabThera, for lymphoma) which have greatly improved the outcomes for patients with these conditions.
Auckland Regional Tissue Bank
In June 2009 the Centre for Clinical Research and effective practice (CCRep) officially launched the Middlemore Tissue Bank (MTB) and began the journey of creating a comprehensive tissue bank at Middlemore Hospital in Auckland. The MTB will potentially serve the North Island of New Zealand and will collaborate closely with the Cancer Society Tissue Bank in Christchurch.
Building upon the enthusiastic support of Auckland’s clinical and academic community the team will seek collaborations with NZ’s academic, research and public health institutions. The Middlemore Tissue Bank looks forward to supporting cutting-edge research projects which will deliver real benefits to NZ’s unique patient population with its diverse ethnicities.
Click here for more information.
The Cancer Society Tissue Bank – Christchurch
This tissue bank was established in 1996 by a group of scientists and clinicians from Christchurch Hospital and the University of Otago, Christchurch Medical School. This group recognised the importance of using human cancer tissues for research and the need for a collection, storage, use and disposal process, that guaranteed patients privacy and confidentiality.
The bank is a collaboration between the Cancer Society of New Zealand, the Canterbury District Health Board and the University of Otago, Christchurch. To date, 5,000 patients have become donors representing all ethnicities. A number of donors have donated samples multiple times over the course of their disease and treatment.
Samples are sent to researchers throughout New Zealand after approval from ethics and the Tissue Bank Board. The complex set of samples required to answer some research questions can only be achieved by using samples already stored in the tissue bank. In this way the Cancer Society Tissue Bank helps to ensure that New Zealand cancer researchers using our resource maintain their international competitiveness.
For more information or to enquire about contributing to a tissue bank in New Zealand, please speak to your treating doctor or contact Leukaemia & Blood Cancer New Zealand.
Lymphoma is not one cancer but refers to many different malignancies which all originate from lymphocytes, which are white blood cells that play an important role in our immune system. Humans have 3 main types of lymphocytes: T-cells, B-cells and NK cells, however within each of these groups many subsets of lymphocytes are defined, an of which may cause lymphoma.
Overall lymphoma is a relatively common cancer, diagnosed in approximately 800 New Zealanders every year; however some lymphomas are very rare. Immune suppression, autoimmune diseases, ageing, ethnicity, radiation exposure and certain infections (viral and bacterial are known to predispose to some types of lymphomas; however in most patients no cause for their lymphoma is identified. Familial (i.e. genetic or inherited) lymphomas are rare.
Lymphoma can arise in any part of the body, although usually lymph nodes are involved. Patients can present with a huge variety of signs and symptoms which can often mimic other diseases; therefore recognising lymphoma can be challenging and patients are occasionally frustrated by multiple tests and a delay in diagnosis. Conversely, many patients with low grade lymphomas have no symptoms and enlarged lymph nodes are found incidentally when scans or blood tests are performed for other indications.
A definitive diagnosis of lymphoma is made by performing several types of tests on a biopsy of the involved tissue. Over 50 types of lymphoma are known, and as the treatment and prognosis of each type of lymphoma may vary considerably, it is vital to obtain an accurate diagnosis. When a diagnosis of lymphoma is established, staging investigations determine the extent of lymphoma throughout the body. Staging contributes to treatment planning and helps predict outcome. Staging investigations include a “full body” CT scan, bone marrow biopsy, and blood tests – including testing for some viral infections. Occasionally special scans (such as MRI or PET) or a lumbar puncture may be required. Unlike other types of cancer it is not only the stage which predicts prognosis and in some case even very advanced disease is considered curable.
Lymphoma staging:
Stage I Single nodal area or structure
Stage II Two or more nodal areas on the same side of the diaphragm
Stage III Nodal areas on both sides of the diaphragm
Stage IV Extranodal involvement
B Symptoms Fever >38°C, weight loss >10% in the preceding 6 months, drenching night sweats

The type of lymphoma/biopsy results, staging investigations and patient’s overall heath determine the treatment options, which may include monitoring only (for low grade disease), radiotherapy, chemotherapy, bone marrow/stem cell transplant and supportive care (such as blood transfusions). Some types of lymphomas have high cure rates while others are considered incurable. Many lymphomas have a validated prognostic scoring system which can help in predicting outcomes.
Lymphoma classification:
There are several components to lymphoma classification. The following information is not exhaustive but outlines the basic framework for classification. Comprehensive diagnostic criteria for lymphoma have been published by the World Health Organisation.
1. The type of lymphocyte involved: In Hodgkin lymphoma, unique malignant B-lymphocytes called Reed-Sternburg and Hodgkin cells are seen. These cells are not found in any other types of lymphomas, which are therefore referred to as non-Hodgkin lymphomas (NHL). NHL is further classified as to the type of lymphocyte involved e.g. B-cell vs T-cell.
2. The site of lymphoma: For example, central nervous system lymphoma or cutaneous (skin) lymphoma
3. The rate of growth: Although there are exceptions to this rule, typically fast growing or aggressive tumours are composed of large lymphoma cells, while slow growing or indolent lymphomas are most often composed of small cells.
B-cell non-Hodgkin lymphomas are the most common types of lymphoma, in particular follicular lymphoma, (an indolent lymphoma) and diffuse large B-cell lymphoma, an aggressive lymphoma.
Frequencies of the more common subtypes of non-Hodgkin lymphoma:


Hodgkin Lymphoma
Hodgkin lymphoma, although, less common than other lymphomas, has its own unique aspects. Typical presentations are enlarged lymph nodes in the neck or within the chest. About 20% of patients also have fevers, sweats or skin itch at the time of diagnosis.
The requirement to biopsy the enlarged nodes and perform CT scans and bone marrow biopsies, in some cases, is similar to other lymphomas.
Hodgkin lymphoma occurs more frequently in younger patients than other lymphomas posing unique issues relating to preservation of fertility and minimizing the long term side effects of treatment. Fortunately, current treatment using combination chemotherapy and radiotherapy has a high cure rate and fertility is usually preserved. Clinical trials are currently focusing on minimizing treatment in good risk disease and intensifying treatment in poor risk disease. Patients with recurrent disease may still be cured with an autologous stem cell transplant.
More information
For more information about the different subtypes of lymphoma, including patient information booklets, please click here.
Leukaemia & Blood Cancer New Zealand (LBC) is a registered provider of Continuing Medical Education (CME) credits with the Royal New Zealand College of General Practitioners (RNZCGP).
As such, we are committed to developing a programme of education sessions for GPs (and practice nurses) around New Zealand in the coming years.
On average, a New Zealand GP may encounter seven to eight lymphoma patients during their career*. LBC is committed to increasing awareness of lymphoma and its signs and symptoms with GPs and practice nurses. We have recently created several lymphoma-specific resources for GPs:
Is Lymphoma on Your Radar? – a double-sided diagnostic decision tool card with flow chart and list of signs, symptoms and initial investigations when lymphoma is suspected.
Early Diagnosis and Referral of Lymphoma is Critical – an article co-authored by Dr Peter Browett, Medical Director, Leukaemia & Blood Cancer New Zealand and Dr Ken Bradstock, Westmead Hospital, Sydney.
Understanding Lymphoma both available as a wall poster and an A4 tear-off pad, this one-stop overview of the types and treatments of lymphoma is popular with GPs and specialist clinics alike.
Non-Hodgkin Lymphoma and Hodgkin_Lymphoma patient information booklets
Tom has Lymphoma picture book for paediatric patients and children of adult patients
Lymphoma Today twice yearly newsletter for patients and families living with lymphoma
*Based on current diagnostic statistics, the number of GPs in New Zealand and an average career length of 30 years.
There is a list of clinical trials currently available in New Zealand in lymphoma, available on the “ClinTrial Refer” app.
Android Device click here
Apple App Store click here

Tissue banks (also known as tumour banks) are a useful research resource. They collect, process, store and subsequently provide cancerous tissues and cells (including blood and bone marrow) for ethically approved research studies. This may be in the form of solid tumours (e.g. lymphoma or breast cancer), bone marrow and blood (e.g. leukaemia, myeloma) that is being collected in a routine biopsy or blood test.
Specially trained medical professionals will provide you with full information regarding the tissue bank, obtain informed consent, collect and prepare the samples for storage as well as record comprehensive, de-identified, clinical information about each donor and the corresponding sample(s). Tissue banks have become an integral part of many state-of-the-art hospitals and cancer centres across the world.
The tumour samples and associated clinical data are important resources for scientists engaged in molecular research to develop better diagnostic tools and new drug therapies. Results from this type of research have been successful in recent times leading to the development of targeted therapies such as Imatinib (also known as Glivec, for chronic myeloid leukaemia) and Rituximab (also known as MabThera, for lymphoma) which have greatly improved the outcomes for patients with these conditions.
Auckland Regional Tissue Bank
In June 2009 the Centre for Clinical Research and effective practice (CCRep) officially launched the Middlemore Tissue Bank (MTB) and began the journey of creating a comprehensive tissue bank at Middlemore Hospital in Auckland. The MTB will potentially serve the North Island of New Zealand and will collaborate closely with the Cancer Society Tissue Bank in Christchurch.
Building upon the enthusiastic support of Auckland’s clinical and academic community the team will seek collaborations with NZ’s academic, research and public health institutions. The Middlemore Tissue Bank looks forward to supporting cutting-edge research projects which will deliver real benefits to NZ’s unique patient population with its diverse ethnicities.
Click here for more information.
The Cancer Society Tissue Bank – Christchurch
This tissue bank was established in 1996 by a group of scientists and clinicians from Christchurch Hospital and the University of Otago, Christchurch Medical School. This group recognised the importance of using human cancer tissues for research and the need for a collection, storage, use and disposal process, that guaranteed patients privacy and confidentiality.
The bank is a collaboration between the Cancer Society of New Zealand, the Canterbury District Health Board and the University of Otago, Christchurch. To date, 5,000 patients have become donors representing all ethnicities. A number of donors have donated samples multiple times over the course of their disease and treatment.
Samples are sent to researchers throughout New Zealand after approval from ethics and the Tissue Bank Board. The complex set of samples required to answer some research questions can only be achieved by using samples already stored in the tissue bank. In this way the Cancer Society Tissue Bank helps to ensure that New Zealand cancer researchers using our resource maintain their international competitiveness.
For more information or to enquire about contributing to a tissue bank in New Zealand, please speak to your treating doctor or contact Leukaemia & Blood Cancer New Zealand.
Information in this section is restricted to members who are logged in to the site.
Please click here
The value of the internet is widely recognised, however, not all the information available may be accurate and up to date. For this reason, we have selected some of the key sites that people living with lymphoma might find useful.
With the exception of our own websites, Leukaemia & Blood Cancer New Zealand (LBC) does not maintain these listed sites. We have only suggested sites we believe may offer credible and responsible information, but we cannot guarantee the information on them is correct, up to date or evidence based medical information.
If you have a specific query about lymphoma that this site has been unable to answer, please email Leukaemia & Blood Cancer New Zealand at info@leukaemia.org.nz.
Leukaemia & Blood Cancer New Zealand
www.leukaemia.org.nz
EVIQ
www.eviq.org.au
Leukaemia Foundation of Australia
www.leukaemia.org.au
Cancer Society of New Zealand
www.cancernz.org.nz
Lymphoma Coalition
www.lymphomacoalition.org
HSANZ – the Haematology Society of Australia and New Zealand
www.hsanz.org.au